














[Body Building]
[ChildLife Products]
[Childrens Health & Wellbeing]
[General Health]
[Sexual Health]
[Sleep Support]
[Weight Management]
[FAQ]
[Price List]
[Reviews]
[Specials]
[Top Products]
[Supplement Overview]
[Club Page]
[What]
[NEW PRODUCT]
NATURAL CARE PRODUCTS
Gisborne New Zealand
Gisborne New Zealand

This site uses E-Commerce from






NO PAYPAL ACCOUNT REQUIRED

Arthritis - Rheumatoid Diagnosis
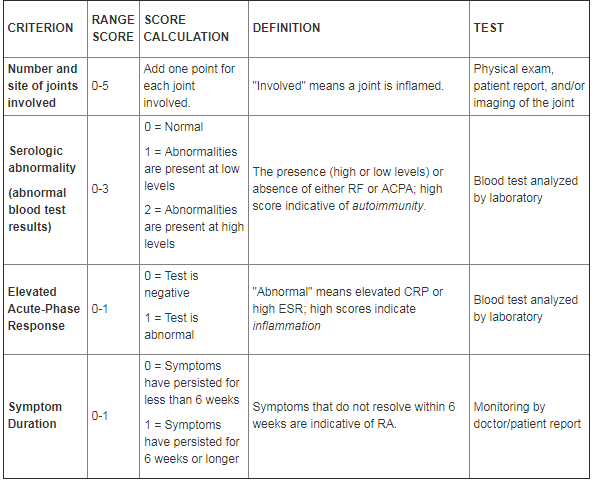
The two important factors to consider when diagnosing RA are 1) whether inflammation is present, and 2) whether an autoimmune response is occurring. Inflammation can be measured with a variety of blood tests including hs-CRP (measures inflammation quantitatively) and an erythrocyte sedimentation rate (ESR) test (measures inflammation functionally) (St. Clair 2004).
To help determine if an autoimmune reaction is taking place, doctors often assess the levels of two proteins: rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA), sometimes referred to as anti-cyclic citrullinated protein (anti-CCP). Both RF and ACPA are autoantibodies involved in the immune attack against self-tissue in RA.
Table 1. Criteria for a definitive diagnosis of rheumatoid arthritis.> A definitive diagnosis requires confirming synovitis due to RA in at least one joint. Additionally, a total score = 6 by adding the individual criterion scores below (Aletaha 2010; Pietschmann 2011).
To help determine if an autoimmune reaction is taking place, doctors often assess the levels of two proteins: rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA), sometimes referred to as anti-cyclic citrullinated protein (anti-CCP). Both RF and ACPA are autoantibodies involved in the immune attack against self-tissue in RA.
Table 1. Criteria for a definitive diagnosis of rheumatoid arthritis.> A definitive diagnosis requires confirming synovitis due to RA in at least one joint. Additionally, a total score = 6 by adding the individual criterion scores below (Aletaha 2010; Pietschmann 2011).
The goal of RA treatment is to prevent and/or control joint damage, prevent loss of function, and decrease pain (American College of Rheumatology 2002). Early diagnosis and treatment is important for achieving the best possible outcome (Nell 2004; van Aken 2004).
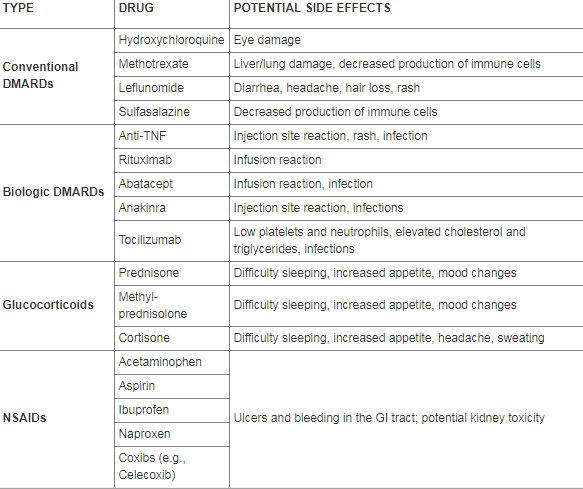
To date, conventional medicine has relied on a mix of powerful pharmaceuticals designed to slow the disease process. While these drugs have been shown to provide relief for many patients, they may also cause side effects that can seriously reduce quality of life. Typically, treatment with one or more of the following types of prescription drugs begins as soon as the diagnosis is confirmed.
Disease-Modifying Antirheumatic Drugs (DMARDS)
DMARDSs decrease joint inflammation and slow the progression of joint damage (Ma 2010).
The two principle classes of DMARDs are conventional and biologic. Conventional DMARDs are chemically synthesized and suppress the immune system. Biologic DMARDs are genetically engineered to target specific molecules of the immune system.
Examples of conventional DMARDs include methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine. Methotrexate (often the DMARD of choice used to treat established RA) is sometimes used in combination with other drugs, including other DMARDs to reduce disease activity as much as possible (Jurgens 2011).
Biologic DMARDs are newer than conventional DMARDs. They are considered second-line drugs after conventional DMARDS for the treatment of RA. Examples of biologic DMARDs include drugs that target TNF-a (a potent pro-inflammatory mediator produced in large amounts in RA). Some anti-TNF-a drugs include adalimumab, etanercept, and certolizumab pegol. Since TNF-a orchestrates the inflammatory network that drives so many disease processes, some DMARDs are being used experimentally for conditions in which autoimmunity is not a central feature. For example, entanercept (Enbrel®) is being explored as a potential therapeutic agent for Alzheimer's disease (Life Extension 2012).
Another commonly prescribed biologic DMARD targeting ß-cells (the immune cell that produces antibodies) is rituximab. Rituximab has been shown to reduce RA related symptoms such as joint damage (Edwards 2004; Keystone 2009). Other biologic DMARDSs include abatacept, an inhibitor of T-cell activation and tocilizumab, an antibody against the IL-6 receptor (Tak 2011).
Glucocorticoids
Glucocorticoids suppress both inflammation and the activity of immune system cells. The most commonly used glucocorticoids today are prednisone and methylprednisolone (a more potent glucocorticoid than prednisone). When administered systemically, these drugs can be effective but can also cause side effects (e.g., osteoporosis, eye disease, insomnia, weight gain, and increased susceptibility to infection), which can dramatically impact quality of life (American College of Rheumatology 2002; Moreland 2002). Even though glucocorticoids can be injected directly into the affected joint, the benefits of this delivery method are temporary (American College of Rheumatology 2002).
Doctors often use prednisone as a "bridging" therapy after patients are diagnosed with RA. This regimen includes the use of prednisone for six to twelve months to allow DMARDs to take effect (St. Clair 2004; van Gestel 1995).
Chronotherapy - European Method Dramatically Reduces Morning Stiffness in RA
It is well known that the immune system displays diurnal variation; that is, it fluctuates depending upon the time of day.
Beginning around midnight, levels of the inflammatory mediators TNF-a and IL-6 rise sharply and peak in the early morning hours (Cutolo 2011; Straub 2007). This nocturnal inflammatory exacerbation underlies the early morning disease flares characteristic of rheumatoid arthritis and represents an opportunity for the emerging field of chronotherapeutics - biorhythmically targeted treatments.
Recently, a modified-release delivery method for prednisone has been developed. This form of prednisone is taken at bedtime (10 PM) and releases into the bloodstream at approximately 2 AM. This is important because conventional prednisone formulations only suppress inflammation for a few hours, making it difficult to target inflammation late at night.
In clinical trials, this modified-release prednisone has been shown to dramatically reduce the duration of morning stiffness (-22.7% vs. -0.4%) and suppress levels of the inflammatory mediator IL-6 (- 29% vs. no change) compared to conventional prednisone (Buttgereit 2010; Buttgereit 2011). Modified-release prednisone also improved overall disease activity more than standard formulations of prednisone.
Unfortunately, the United States FDA recently denied the request of a European drug maker to import a branded formulation of modified-release prednisone called Lodotra® (http://www.accessdata.fda.gove/scripts/importrefusals/ir_detail.cfm?EntryId=UPS-2301487-7&DocId=1&LineId=1&SfxId=). However, after successfully achieving treatment goals in two RA clinical trials in the US, the manufacturer of Lodotra®, Horizon Pharma, submitted a New Drug Application to the FDA in Late 2011. Approval is pending, but expected relatively soon.
This advanced prednisone delivery system promises to fill a gap in current RA treatment regimens. By targeting nighttime inflammation and relieving morning disease flares, RA patients can hope to experience a considerable improvement in their quality of life.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDS)
NSAIDs inhibit inflammation and reduce pain. This class of drugs operates by inhibiting the pro-inflammatory enzymes cyclooxygenase-1 and -2 (COX-1 and COX-2). Both of the COX enzymes convert arachidonic acid (an omega-6 fatty acid) into pro-inflammatory prostaglandins, which contribute to swelling and pain.
Selective COX-2 inhibitors were revolutionary when introduced-but then grave side effects were discovered (St. Clair 2004; Trelle 2011). The NSAID rofecoxib (Vioxx®) after being prescribed to tens of thousands of RA patients was removed from the market in 2004 when it was shown to significantly increase risk of heart attack and stroke. Other COX-2 inhibitors such as valdecoxib (Bextra®) were voluntarily removed from the market after studies revealed similar risks. Years before the public learned about the dangers of Vioxx® and Bextra®, Life Extension warned its customers that taking these drugs would create lethal havoc in the body (Faloon 2001). Currently, only one COX-2 inhibitor-Celebrex®-is available on the U.S. market.
The remaining NSAIDs on the market inhibit both the COX-1 and COX-2 enzymes. Unfortunately, these can lead to gastrointestinal side effects such as pain and bleeding because COX-1 is important for proper functioning of the gastrointestinal mucosa.
Additional NSAIDs include aspirin, naproxen, ibuprofen, and acetaminophen. Aspirin inhibits the aggregation of platelets (the components of blood that "clump together" and form a blood clot) more so than other NSAIDs. Taking low-dose aspirin may be beneficial for those at a higher risk of cardiovascular disease (Pearson 2002). However, taking aspirin in combination with therapeutic doses of the common RA drug methotrexate may cause liver and kidney damage (Colebatch 2011).
Statins
Because the chief cause of mortality among people with RA is cardiovascular disease, keeping cholesterol levels within a healthy range is an important component of treatment. Statin drugs have been shown to effectively lower cholesterol levels up to 16% as well as significantly reduce cardiovascular events (e.g., heart attacks) in people with rheumatoid arthritis (Sheng 2011; Ridker 2009).
Although statins are widely prescribed, they have many potential side effects including a breakdown of muscle tissue. Statins are also known to cause depletion of coenzyme Q10, which is necessary for basic cell function. Patients taking statins should supplement with coenzyme Q10 to avoid depletion of this critical enzyme. Life Extension suggests that CoQ10 blood levels be kept in the range of 3 - 7 µg/mL.
Table 2. Types of conventional medicines used in the treatment of rheumatoid arthritis and their potential side effects (Kahlenberg 2011; American College of Rheumatology 2002; Ma 2010; Moreland 2002; Youssef 1997; McCormack 2011; Coblyn 2011)
To date, conventional medicine has relied on a mix of powerful pharmaceuticals designed to slow the disease process. While these drugs have been shown to provide relief for many patients, they may also cause side effects that can seriously reduce quality of life. Typically, treatment with one or more of the following types of prescription drugs begins as soon as the diagnosis is confirmed.
Disease-Modifying Antirheumatic Drugs (DMARDS)
DMARDSs decrease joint inflammation and slow the progression of joint damage (Ma 2010).
The two principle classes of DMARDs are conventional and biologic. Conventional DMARDs are chemically synthesized and suppress the immune system. Biologic DMARDs are genetically engineered to target specific molecules of the immune system.
Examples of conventional DMARDs include methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine. Methotrexate (often the DMARD of choice used to treat established RA) is sometimes used in combination with other drugs, including other DMARDs to reduce disease activity as much as possible (Jurgens 2011).
Biologic DMARDs are newer than conventional DMARDs. They are considered second-line drugs after conventional DMARDS for the treatment of RA. Examples of biologic DMARDs include drugs that target TNF-a (a potent pro-inflammatory mediator produced in large amounts in RA). Some anti-TNF-a drugs include adalimumab, etanercept, and certolizumab pegol. Since TNF-a orchestrates the inflammatory network that drives so many disease processes, some DMARDs are being used experimentally for conditions in which autoimmunity is not a central feature. For example, entanercept (Enbrel®) is being explored as a potential therapeutic agent for Alzheimer's disease (Life Extension 2012).
Another commonly prescribed biologic DMARD targeting ß-cells (the immune cell that produces antibodies) is rituximab. Rituximab has been shown to reduce RA related symptoms such as joint damage (Edwards 2004; Keystone 2009). Other biologic DMARDSs include abatacept, an inhibitor of T-cell activation and tocilizumab, an antibody against the IL-6 receptor (Tak 2011).
Glucocorticoids
Glucocorticoids suppress both inflammation and the activity of immune system cells. The most commonly used glucocorticoids today are prednisone and methylprednisolone (a more potent glucocorticoid than prednisone). When administered systemically, these drugs can be effective but can also cause side effects (e.g., osteoporosis, eye disease, insomnia, weight gain, and increased susceptibility to infection), which can dramatically impact quality of life (American College of Rheumatology 2002; Moreland 2002). Even though glucocorticoids can be injected directly into the affected joint, the benefits of this delivery method are temporary (American College of Rheumatology 2002).
Doctors often use prednisone as a "bridging" therapy after patients are diagnosed with RA. This regimen includes the use of prednisone for six to twelve months to allow DMARDs to take effect (St. Clair 2004; van Gestel 1995).
Chronotherapy - European Method Dramatically Reduces Morning Stiffness in RA
It is well known that the immune system displays diurnal variation; that is, it fluctuates depending upon the time of day.
Beginning around midnight, levels of the inflammatory mediators TNF-a and IL-6 rise sharply and peak in the early morning hours (Cutolo 2011; Straub 2007). This nocturnal inflammatory exacerbation underlies the early morning disease flares characteristic of rheumatoid arthritis and represents an opportunity for the emerging field of chronotherapeutics - biorhythmically targeted treatments.
Recently, a modified-release delivery method for prednisone has been developed. This form of prednisone is taken at bedtime (10 PM) and releases into the bloodstream at approximately 2 AM. This is important because conventional prednisone formulations only suppress inflammation for a few hours, making it difficult to target inflammation late at night.
In clinical trials, this modified-release prednisone has been shown to dramatically reduce the duration of morning stiffness (-22.7% vs. -0.4%) and suppress levels of the inflammatory mediator IL-6 (- 29% vs. no change) compared to conventional prednisone (Buttgereit 2010; Buttgereit 2011). Modified-release prednisone also improved overall disease activity more than standard formulations of prednisone.
Unfortunately, the United States FDA recently denied the request of a European drug maker to import a branded formulation of modified-release prednisone called Lodotra® (http://www.accessdata.fda.gove/scripts/importrefusals/ir_detail.cfm?EntryId=UPS-2301487-7&DocId=1&LineId=1&SfxId=). However, after successfully achieving treatment goals in two RA clinical trials in the US, the manufacturer of Lodotra®, Horizon Pharma, submitted a New Drug Application to the FDA in Late 2011. Approval is pending, but expected relatively soon.
This advanced prednisone delivery system promises to fill a gap in current RA treatment regimens. By targeting nighttime inflammation and relieving morning disease flares, RA patients can hope to experience a considerable improvement in their quality of life.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDS)
NSAIDs inhibit inflammation and reduce pain. This class of drugs operates by inhibiting the pro-inflammatory enzymes cyclooxygenase-1 and -2 (COX-1 and COX-2). Both of the COX enzymes convert arachidonic acid (an omega-6 fatty acid) into pro-inflammatory prostaglandins, which contribute to swelling and pain.
Selective COX-2 inhibitors were revolutionary when introduced-but then grave side effects were discovered (St. Clair 2004; Trelle 2011). The NSAID rofecoxib (Vioxx®) after being prescribed to tens of thousands of RA patients was removed from the market in 2004 when it was shown to significantly increase risk of heart attack and stroke. Other COX-2 inhibitors such as valdecoxib (Bextra®) were voluntarily removed from the market after studies revealed similar risks. Years before the public learned about the dangers of Vioxx® and Bextra®, Life Extension warned its customers that taking these drugs would create lethal havoc in the body (Faloon 2001). Currently, only one COX-2 inhibitor-Celebrex®-is available on the U.S. market.
The remaining NSAIDs on the market inhibit both the COX-1 and COX-2 enzymes. Unfortunately, these can lead to gastrointestinal side effects such as pain and bleeding because COX-1 is important for proper functioning of the gastrointestinal mucosa.
Additional NSAIDs include aspirin, naproxen, ibuprofen, and acetaminophen. Aspirin inhibits the aggregation of platelets (the components of blood that "clump together" and form a blood clot) more so than other NSAIDs. Taking low-dose aspirin may be beneficial for those at a higher risk of cardiovascular disease (Pearson 2002). However, taking aspirin in combination with therapeutic doses of the common RA drug methotrexate may cause liver and kidney damage (Colebatch 2011).
Statins
Because the chief cause of mortality among people with RA is cardiovascular disease, keeping cholesterol levels within a healthy range is an important component of treatment. Statin drugs have been shown to effectively lower cholesterol levels up to 16% as well as significantly reduce cardiovascular events (e.g., heart attacks) in people with rheumatoid arthritis (Sheng 2011; Ridker 2009).
Although statins are widely prescribed, they have many potential side effects including a breakdown of muscle tissue. Statins are also known to cause depletion of coenzyme Q10, which is necessary for basic cell function. Patients taking statins should supplement with coenzyme Q10 to avoid depletion of this critical enzyme. Life Extension suggests that CoQ10 blood levels be kept in the range of 3 - 7 µg/mL.
Table 2. Types of conventional medicines used in the treatment of rheumatoid arthritis and their potential side effects (Kahlenberg 2011; American College of Rheumatology 2002; Ma 2010; Moreland 2002; Youssef 1997; McCormack 2011; Coblyn 2011)
Stem Cells - A Developing Strategy for RA Treatment
Stem cells are unique in that they can either divide and reproduce or differentiate into specialized cells. The therapeutic potential of stem cells is a very hot topic in clinical research today. For example, scientists are testing ways to induce a stem cell to turn into normal nerve cells, and then implanting them to replace dead cells in people who have been paralyzed.
Stem cells can be treated in the laboratory to develop into cartilage, bone, and muscle cells, all of which can be damaged through RA mediated inflammation (Dudics 2009; Duijnisveld 2011).
As of 2011, 89 people with RA have received therapeutic stem cell transplants in hopes of causing disease remission or at a minimum, improvement. One study analyzed the result of high-dose chemotherapy in combination with a stem cell transplant in 7 patients with RA. Assessment of disease activity indicated that 5 (71.4%) of the patients clinically responded to this treatment, meaning that symptoms improved. However, stem cell transplants are associated with a treatment related mortality (TRM) of approximately 5-10%. Therefore, this treatment is reserved for only the most severe cases (Tyndall 2011).
Stem cells are unique in that they can either divide and reproduce or differentiate into specialized cells. The therapeutic potential of stem cells is a very hot topic in clinical research today. For example, scientists are testing ways to induce a stem cell to turn into normal nerve cells, and then implanting them to replace dead cells in people who have been paralyzed.
Stem cells can be treated in the laboratory to develop into cartilage, bone, and muscle cells, all of which can be damaged through RA mediated inflammation (Dudics 2009; Duijnisveld 2011).
As of 2011, 89 people with RA have received therapeutic stem cell transplants in hopes of causing disease remission or at a minimum, improvement. One study analyzed the result of high-dose chemotherapy in combination with a stem cell transplant in 7 patients with RA. Assessment of disease activity indicated that 5 (71.4%) of the patients clinically responded to this treatment, meaning that symptoms improved. However, stem cell transplants are associated with a treatment related mortality (TRM) of approximately 5-10%. Therefore, this treatment is reserved for only the most severe cases (Tyndall 2011).
ARTHRITIS PAGE