














[Body Building]
[ChildLife Products]
[Childrens Health & Wellbeing]
[General Health]
[Sexual Health]
[Sleep Support]
[Weight Management]
[FAQ]
[Price List]
[Reviews]
[Specials]
[Top Products]
[Supplement Overview]
[Club Page]
[What]
[NEW PRODUCT]
NATURAL CARE PRODUCTS
Gisborne New Zealand
Gisborne New Zealand

This site uses E-Commerce from






NO PAYPAL ACCOUNT REQUIRED

More NEWS on Rheumatoid Arthritis
Arthritis - Rheumatoid Symptoms And Affected Tissues
The prominent feature of rheumatoid arthritis is joint inflammation. Affected joints are usually swollen, warm, painful and stiff. These symptoms typically worsen in the morning but, at least early in the disease process, can sometimes be eased by gentle movement. As the disease progresses, however, these symptoms often increase in severity until movement is severely impaired.
Inflammation associated with RA is systemic, meaning that it is not isolated to only those joints affected. RA tends to present symptoms in a symmetrical way. For example, if the joints of the right hand are inflamed, the joints of the left hand are likely to be inflamed as well (St. Clair 2004). While the hand and wrist joints are most often affected, other joints may be involved including those of the feet and ankles, knees, hips, elbows, shoulders, and the cervical spine (i.e., the neck) (Klippel 2010).
Inflammation associated with RA is systemic, meaning that it is not isolated to only those joints affected. RA tends to present symptoms in a symmetrical way. For example, if the joints of the right hand are inflamed, the joints of the left hand are likely to be inflamed as well (St. Clair 2004). While the hand and wrist joints are most often affected, other joints may be involved including those of the feet and ankles, knees, hips, elbows, shoulders, and the cervical spine (i.e., the neck) (Klippel 2010).
In general, the symptoms and severity of RA follow one of three patterns (Ruffing 2012):
Spontaneous remission: The symptoms ultimately disappear, which occurs in less than 10%
of patients with RA. This generally occurs only in patients whose blood tests are negative for
a protein called rheumatoid factor (RF), an autoimmune mediator.
Relapsing/remitting disease: The patient experiences periods of very severe symptoms
called "flares", which are contrasted with episodes of mild or no symptoms. This pattern
generally occurs early on in the course of the disease. Persistent and progressive disease:
Disease activity gets progressively worse. However, flares and periods of remission are not
as dramatic as relapsing/remitting disease. This is the most common course of disease.
During the course of the disease process, RA mediated inflammation can cause permanent
damage to several tissues in the body, especially the joints (NIAMS 2009).
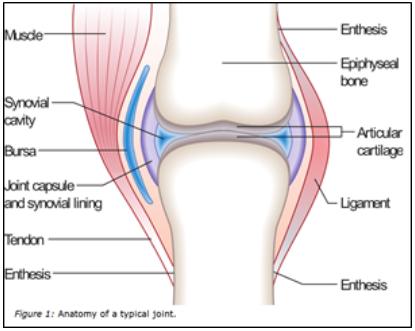
In RA, the immune system mistakenly attacks healthy cells and tissues - predominantly the
synovium, the soft tissue between the articular capsule (joint capsule) and the joint cavity of
synovial joints. This immune mediated assault leads to the development of pannus, a
destructive fibrous tissue within affected joints that erodes cartilage and exacerbates joint
dysfunction.
RA damage is engendered by multiple components of the immune system, including antibodies and killer T-cells.
Antibodies are proteins secreted by ß-cells that normally recognize and bind to invading microbes such as bacteria and viruses. By attaching to the invading microbe, they activate other components of the immune system to launch an inflammatory response, which destroys the cells.
How Autoimmune Inflammation Destroys Joints
In RA, antibodies mistakenly recognize "self" cells as invaders. Once antibodies attach to synovial cells in the joint, they attract a variety of immune cells that launch a devastating inflammatory attack. The complex inflammatory process within joints is mediated in large by the cytokines tumor necrosis factor-alpha (TNF-a) and interleukin-6 (IL-6). The inflammatory damage is not limited to the synovium, but spills over to the chondrocytes (cartilage cells that cushion joints). This process raises the level of dangerous inflammatory compounds throughout the body, including C-reactive protein (CRP), which is a marker of inflammation and can be evaluated via a high-sensitivity CRP (hs-CRP) test.
Another kind of immune system cell that develops in the thymus and contributes to RA is the T-cell. One T-cell sub-type-the "killer" T-cell-can directly kill other cells. This is useful in eradicating invading microbes, but in the case of RA, killer T-cells contribute to tissue damage by directly damaging joints and other affected organs.
An important pathological feature of arthritis is the exposure of collagen as a result of cartilage deterioration. When a joint is sufficiently damaged, collagen (a protein component of cartilage) becomes exposed to circulating immune cells, which attack it. This process promotes further inflammatory joint destruction.
Under normal circumstances, joint tissue can repair itself. However, joints may become permanently weakened and deformed if inflammation is severe, chronic, and occurs over many years as with RA.
Inflammatory Damage Associated with Rheumatoid Arthritis Extends Beyond the Joints.
Once the immune system is activated against self-tissue, it sends inflammatory chemicals through the body resulting in widespread damage. For many patients it causes fatigue, malaise and unexplained weight loss.
Other areas targeted by the immune system in RA can include the skin, lungs, eyes, blood, nervous system, heart, and bones. Signs and symptoms may include (Klippel 2010; St. Clair 2004; Cush 2005):
Skin: Nodules and ulcers on the surface of the skin occur in 50% of people with RA (Mikuls 2007).
Lungs: RA may cause interstitial lung disease, resulting in a dry cough and shortness of breath that may worsen with physical activity; 20-30% of people with RA have some form of lung disease (Kahlenberg 2011).
Eyes: Inflamed eyes are common and affect up to 25% of people with RA. Parts of the eye often targeted include the cornea, conjunctiva, and sclera (the white portion of the eye).
Blood: Anemia and low iron levels often occur in RA and can cause fatigue, fast heartbeat, dizziness and pale skin.
Nervous system: Degeneration of the cervical vertebrae of the spine can compress the spinal cord in the neck area, causing pain on top of that caused by synovitis (inflammation of the synovium).
Heart: People with RA are at a two-fold greater risk of developing heart disease, thus contributing to the 40% greater mortality rate of people with RA compared to the general population (Radovits 2010; Peters 2009). Even early in the disease process, RA patients are prone to endothelial dysfunction due to increased circulating inflammatory molecules. Endothelial cells are the delicate cells lining the inside of blood vessels. Endothelial dysfunction is the initial stage of potentially fatal atherosclerotic vascular disease (Tanasescu 2009).
Bones: People with RA have a significantly increased risk of bone fractures. Both the disease and medicine(s) used to treat RA (e.g., corticosteroids) can cause bone loss, which increases the risk of bone fractures (Spector 1993).
Dyslipidemia: People who have RA are more likely to have dyslipidemia (elevated levels of cholesterol and triglycerides in blood) (Park 1999; Boers 2003). One study showed dyslipidemia 10 years before the development of RA (van Halm 2007). Therefore, it is important that people with both dyslipidemia and a family history of RA focus on prevention and monitor their health very closely. Dyslipidemia and endothelial dysfunction synergize to dramatically compromise the cardiovascular health of RA patients.
Spontaneous remission: The symptoms ultimately disappear, which occurs in less than 10%
of patients with RA. This generally occurs only in patients whose blood tests are negative for
a protein called rheumatoid factor (RF), an autoimmune mediator.
Relapsing/remitting disease: The patient experiences periods of very severe symptoms
called "flares", which are contrasted with episodes of mild or no symptoms. This pattern
generally occurs early on in the course of the disease. Persistent and progressive disease:
Disease activity gets progressively worse. However, flares and periods of remission are not
as dramatic as relapsing/remitting disease. This is the most common course of disease.
During the course of the disease process, RA mediated inflammation can cause permanent
damage to several tissues in the body, especially the joints (NIAMS 2009).
In RA, the immune system mistakenly attacks healthy cells and tissues - predominantly the
synovium, the soft tissue between the articular capsule (joint capsule) and the joint cavity of
synovial joints. This immune mediated assault leads to the development of pannus, a
destructive fibrous tissue within affected joints that erodes cartilage and exacerbates joint
dysfunction.
RA damage is engendered by multiple components of the immune system, including antibodies and killer T-cells.
Antibodies are proteins secreted by ß-cells that normally recognize and bind to invading microbes such as bacteria and viruses. By attaching to the invading microbe, they activate other components of the immune system to launch an inflammatory response, which destroys the cells.
How Autoimmune Inflammation Destroys Joints
In RA, antibodies mistakenly recognize "self" cells as invaders. Once antibodies attach to synovial cells in the joint, they attract a variety of immune cells that launch a devastating inflammatory attack. The complex inflammatory process within joints is mediated in large by the cytokines tumor necrosis factor-alpha (TNF-a) and interleukin-6 (IL-6). The inflammatory damage is not limited to the synovium, but spills over to the chondrocytes (cartilage cells that cushion joints). This process raises the level of dangerous inflammatory compounds throughout the body, including C-reactive protein (CRP), which is a marker of inflammation and can be evaluated via a high-sensitivity CRP (hs-CRP) test.
Another kind of immune system cell that develops in the thymus and contributes to RA is the T-cell. One T-cell sub-type-the "killer" T-cell-can directly kill other cells. This is useful in eradicating invading microbes, but in the case of RA, killer T-cells contribute to tissue damage by directly damaging joints and other affected organs.
An important pathological feature of arthritis is the exposure of collagen as a result of cartilage deterioration. When a joint is sufficiently damaged, collagen (a protein component of cartilage) becomes exposed to circulating immune cells, which attack it. This process promotes further inflammatory joint destruction.
Under normal circumstances, joint tissue can repair itself. However, joints may become permanently weakened and deformed if inflammation is severe, chronic, and occurs over many years as with RA.
Inflammatory Damage Associated with Rheumatoid Arthritis Extends Beyond the Joints.
Once the immune system is activated against self-tissue, it sends inflammatory chemicals through the body resulting in widespread damage. For many patients it causes fatigue, malaise and unexplained weight loss.
Other areas targeted by the immune system in RA can include the skin, lungs, eyes, blood, nervous system, heart, and bones. Signs and symptoms may include (Klippel 2010; St. Clair 2004; Cush 2005):
Skin: Nodules and ulcers on the surface of the skin occur in 50% of people with RA (Mikuls 2007).
Lungs: RA may cause interstitial lung disease, resulting in a dry cough and shortness of breath that may worsen with physical activity; 20-30% of people with RA have some form of lung disease (Kahlenberg 2011).
Eyes: Inflamed eyes are common and affect up to 25% of people with RA. Parts of the eye often targeted include the cornea, conjunctiva, and sclera (the white portion of the eye).
Blood: Anemia and low iron levels often occur in RA and can cause fatigue, fast heartbeat, dizziness and pale skin.
Nervous system: Degeneration of the cervical vertebrae of the spine can compress the spinal cord in the neck area, causing pain on top of that caused by synovitis (inflammation of the synovium).
Heart: People with RA are at a two-fold greater risk of developing heart disease, thus contributing to the 40% greater mortality rate of people with RA compared to the general population (Radovits 2010; Peters 2009). Even early in the disease process, RA patients are prone to endothelial dysfunction due to increased circulating inflammatory molecules. Endothelial cells are the delicate cells lining the inside of blood vessels. Endothelial dysfunction is the initial stage of potentially fatal atherosclerotic vascular disease (Tanasescu 2009).
Bones: People with RA have a significantly increased risk of bone fractures. Both the disease and medicine(s) used to treat RA (e.g., corticosteroids) can cause bone loss, which increases the risk of bone fractures (Spector 1993).
Dyslipidemia: People who have RA are more likely to have dyslipidemia (elevated levels of cholesterol and triglycerides in blood) (Park 1999; Boers 2003). One study showed dyslipidemia 10 years before the development of RA (van Halm 2007). Therefore, it is important that people with both dyslipidemia and a family history of RA focus on prevention and monitor their health very closely. Dyslipidemia and endothelial dysfunction synergize to dramatically compromise the cardiovascular health of RA patients.
Rheumatoid arthritis is an autoimmune disease characterized by inflammation, joint destruction, disability and significant pain. The study is the first to investigate the role of vitamin D in the development of neuropathic pain among rheumatoid arthritis patients.
The multicenter study included 93 men and women with rheumatoid arthritis, among whom one-third were diagnosed with neuropathic pain according to Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) questionnaire responses. Subjects who had serum 25-hydroxyvitamin vitamin D levels that averaged 20 nanograms per milliliter (ng/mL) and lower were classified as deficient, while those with levels of 30 ng/mL and higher were classified as normal.
Higher LANSS scores were correlated with lower serum levels of vitamin D. Neuropathic pain was 5.8 times more likely to be diagnosed among subjects with vitamin D deficiency compared to those whose levels were normal.
Our study raises awareness of the need to screen for vitamin D deficiency in rheumatoid arthritis patients with neuropathic pain, Hilal Yesil and colleagues write. With a relatively easy, safe and inexpensive vitamin D supplement, patients could have more satisfactory outcomes in the management of neuropathic pain. This approach could decrease the morbidity associated with vitamin D deficiency and prevent unnecessary drug use.
There is a need for further prospective studies to identify new treatment protocols consisting of vitamin D supplementation for neuropathic complaints in vitamin D-deficient rheumatoid arthritis patients, they conclude.
ARTHRITIS PAGE